

Ambulatory Cardiac Monitoring
Modalities – Indications – Recommendations
The standard ECG provides a brief (10 sec) sample of cardiac electrical activity. On the other hand, ambulatory ECG monitoring offers a view of ECG data (single or multiple leads) over an extended period of time, thereby permitting evaluation of dynamic and transient cardiac electrical phenomena.
The 3 main types of cardiac monitors currently available are:
- Holter Monitor.
- Cardiac Event Monitor (CEM), also known as External Loop Recorders.
- Mobile Cardiac Telemetry (MCT), also known as Mobile Cardiac Outpatient Telemetry (MCOT) and Ambulatory Cardiac Telemetry (ACT).
Holter Monitors
- A Holter monitor is generally used for short-term monitoring, usually 24-48 hours, but extended Holter monitoring periods also are available.
- The Holter monitor logs every heartbeat for both symptomatic and asymptomatic arrhythmias and provides full disclosure of recorded data.
Advantages:
- Complete record of heart rhythm.
- Assessment of sinus node function:
- Chronotropic incompetence
- Inappropriate sinus tachycardia
- Postural orthostatic tachycardia syndrome
- Assessment of rate control during atrial fibrillation.
- Assessment of PVCs or PACs burden.
Disadvantages:
- A Holter monitor is generally used for short-term monitoring, requiring symptoms occurring on daily basis. Therefore, Holter monitors are not preferred in patients with less frequent symptoms.
- Absence of real-time data analysis. Arrhythmias can be diagnosed and addressed only after the patient completes the monitoring period and returns the device. This can cause significant delay in the diagnosis and treatment of high-risk arrhythmias.
- Patient noncompliance with symptom logs. This can undermine the ability to correlate symptoms with underlying heart rhythm.
Cardiac Event Monitors
- CEMs are designed to capture heart rhythm at the time of patient-activated symptomatic events during a monitoring period of 3-30 days.
- The CEM constantly records the heart rhythm but does not save or store recorded data until the “Event Button” is pressed by the patient, at which time, the CEM records a specified period before the event and after activation of the device (e.g., 90 seconds prior to and 90 seconds after the “Event Button” is pressed). The recorded event is transmitted back to the monitoring laboratory automatically or by patient (via telephone).
- For example, when a patient with a CEM experiences an episode of symptoms, he presses the event button, and the recording device will record and save only 90 seconds prior to the event and 90 seconds after. ECG data between those events are not saved.
Advantages:
- CEM offers extended period of monitoring (up to 30 days) and, therefore, is preferred to Holter monitors in patients with less frequent symptoms, especially in compliant patients with low-risk, nondebilitating symptoms (e.g., palpitations) and when a comprehensive assessment of all cardiac activity and identification of asymptomatic arrhythmias are not required.
- On-line monitoring of patient-activated transmissions.
Disadvantages:
- CEM requires occurrence of symptoms and patient’s interaction and compliance to activate monitor promptly at the onset of symptoms. Therefore, CEM is not preferred in patients with questionable ability to recognize symptoms, activate the device, and transmit the recording in a timely manner.
- CEM can miss symptomatic arrhythmias if there is a delay in activation by patient after occurrence of symptoms. For example, a patient who has fainting spells may not return to full consciousness and be able to activate the monitor in a timely manner to capture the arrhythmia that caused syncope. Therefore, CEM is not preferred in patients with disabling symptoms.
- Even when the arrhythmia during the patient-activated event is captured, certain clues that enable the physician to establish the accurate diagnosis of the arrhythmia (such as discrimination between supraventricular versus ventricular tachycardia) lie in the pattern of onset and termination of the arrhythmia, which may not be recorded if these events occur before or after the pre-specified recorded period.
- CEM does not provide a comprehensive assessment of all cardiac activity, such as heart rate trends, burden of arrhythmias (e.g., atrial fibrillation, PVCs).
- CEM cannot identify arrhythmias occurring outside the patient-activation window. Therefore, CEM is not preferred when the identification of asymptomatic arrhythmias is important for patient management (such as long pauses, VT, AF episodes that might be truly asymptomatic or might not cause symptoms simply because they might occur while the patient is lying down or during sleep.
- Patient compliance with extended monitoring.
- Skin irritation from adhesive electrodes.
Mobile Cardiac Telemetry
- MCT continuously records and saves heart rhythm data for a period of up to 30 days.
- MCT monitors are the most advanced form of ambulatory cardiac monitoring technologies. MCT automatically detects cardiac arrhythmias and automatically transmits ECG data to the monitoring laboratory in real time via wireless cell phone (with or without patient interaction). In addition to recording and saving symptomatic patient-triggered events, these devices have auto-detect features that will capture asymptomatic (e.g., atrial fibrillation, tachycardia, bradycardia, and pauses) arrhythmias based on detection algorithms.
- The monitoring laboratory that receives the abnormal ECG activity is comprised of trained personnel, with immediate, 24/7/365 access to a physician to review transmitted data and make clinical decisions regarding the patient. Additionally, the monitoring technicians are trained to contact the patient and to activate emergency medical response to assist the patient in case of an emergency.
- Additionally, MCT provides full disclosure of ECG data, heart rate trend analysis, and arrhythmia burden throughout the entire recording period.
Advantages:
- The ability to respond immediately when clinically important events occur is the major advantage of real-time continuous MCT monitoring compared to other forms of ambulatory cardiac monitoring.
- MCT offers continuous recording of heart rhythm (similar to Holter monitors) for extended intervals (up to 30 days). Therefore, they are preferred to Holter monitors in patients with less frequent symptoms.
- Unlike Holter monitors, MCT enables real-time connectivity and monitoring, so that arrhythmias can be identified and addressed promptly. For example, in a patient with cryptogenic stroke who develops an episode of atrial fibrillation on day 2 of the monitoring period, with MCT, the physician is notified of the occurrence of the arrhythmia, and anticoagulation is started promptly afterwards. In contrast, with Holter monitor, the diagnosis and management of atrial fibrillation is not feasible until the patient completes the monitoring period and returns the monitoring device, which can result in significant delay in initiation of important therapies.
- Unlike CEM, MCT enables the detection of both symptomatic and asymptomatic arrhythmias. This capability helps to optimize patient care by enabling early diagnosis and prompt management of serious arrhythmias. For example, in a patient who develops sustained ventricular tachycardia during sleep, CEM would miss this arrhythmia, whereas MCT will automatically identify the arrhythmia and automatically transmit the recording to the monitoring laboratory staff who, if necessary, can alert the physician, contact the patient, and activate emergency services.
- Unlike CEM, MCT does not require patient involvement. Therefore, MCT is preferred when patient cooperation is not reliable (such as elderly patients, especially those with memory deficits). Also, MCT is preferred in patients high-risk or disabling symptoms (e.g., syncope) as the patient might not be able to press the “Event Button” in a timely manner, and the arrhythmia precipitating the symptoms would have been otherwise missed by CEM.
- Unlike CEM, MCT offers full disclosure of cardiac rhythm data throughout the entire recording period. This can provide important information regarding trends of heart rates, burden of arrhythmias (such as atrial fibrillation or PVCs). This is similar to the capability of Holter monitors, but MCT provides these data for much longer periods than that provided by Holter monitors. Full disclosure of rhythm data is also important to establish the true relationship between arrhythmias and symptoms. For example, when a transmission triggered by a patient during an episode shows frequent PVCs, the importance of the PVCs as the cause of symptoms might be questioned if PVCs are also observed to be frequent at many other occasions when the patient was asymptomatic.
Disadvantages:
- Patient compliance with extended monitoring.
- Skin irritation from adhesive electrodes.
Modalities of Ambulatory Cardiac Monitoring
| Holter Monitor | Cardiac Event Monitor | Mobile Cardiac Telemetry | |
|---|---|---|---|
|
Monitoring duration |
1-2 days |
3-30 days |
3-30 days |
|
Patient-activated symptomatic events |
Yes |
Yes |
Yes |
|
Automatic detection of arrhythmic events |
No |
No |
Yes |
|
Immediate data transmission |
No |
Yes |
Yes |
|
Full disclosure of data |
Yes |
No |
yes |
|
Real-time monitoring |
No |
yes |
Yes |
|
Recording |
Continuous recording typically for 1-2 days, and up to 14 days. |
Records only selected sequences (a short period before and after every patient-triggered event) during a monitoring period of up to 30 days |
Continuous recording for up to 30 days |
|
Advantage |
Logs every heartbeat for both symptomatic and asymptomatic arrhythmias |
-Longer monitoring period for less frequent symptoms. – Appropriate for intermittent, low-risk, nondebilitating symptoms |
– Continuous and extended recording – Full disclosure. |
|
Disadvantages |
– Short timeframe: requires symptoms |
– Requires occurrence of symptoms – |
– Patient compliance with extended monitoring.
– Skin irritation from adhesive electrodes.
|
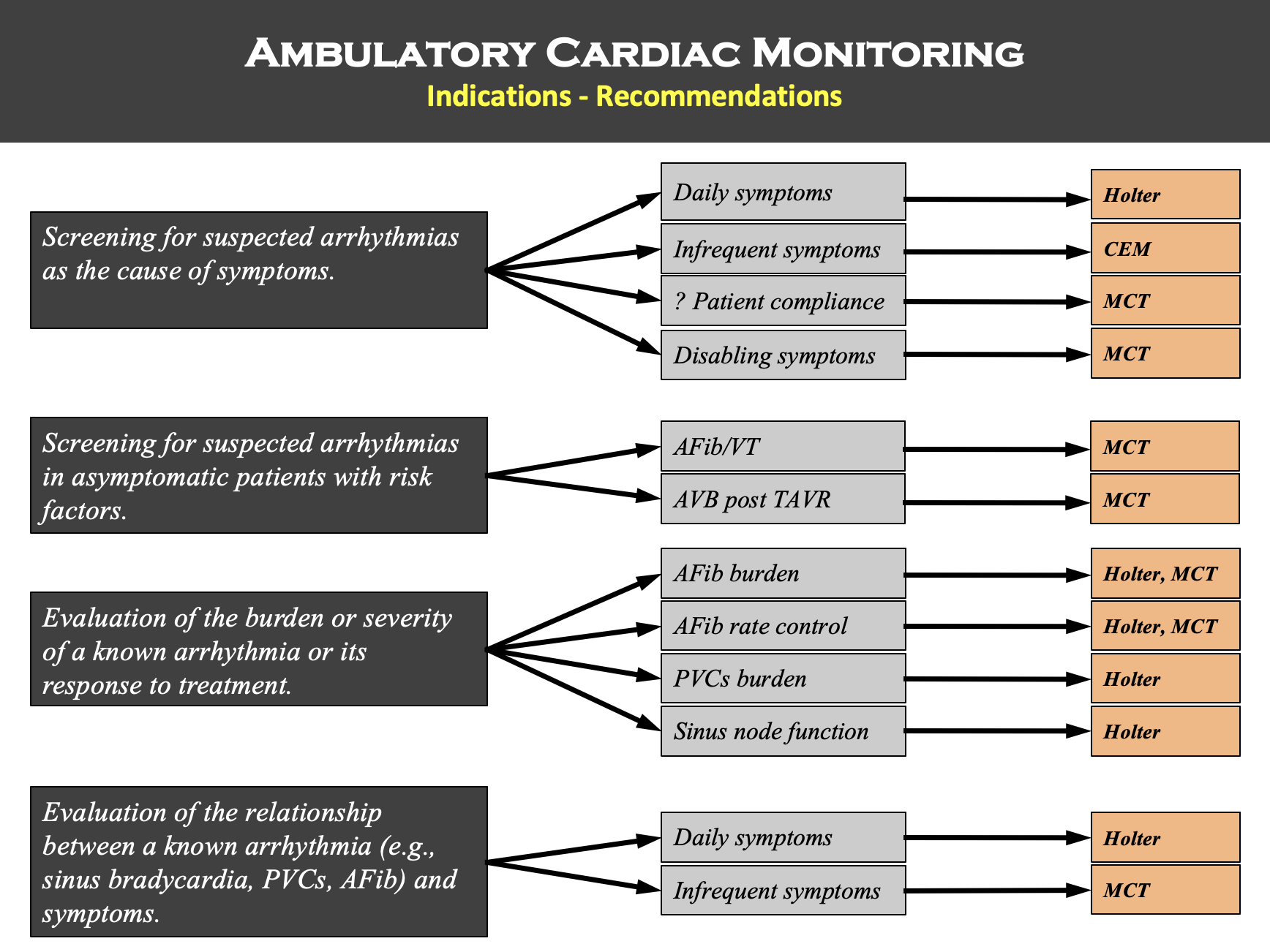
Ambulatory Cardiac Monitoring Indications
1. Evaluation for suspected arrhythmias as the potential cause of symptoms.
Examples:
- Syncope, presyncope, dizziness.
- Palpitations (heart racing, pounding, skipping).
- Ambiguous symptoms (fatigue, dyspnea, chest discomfort, “seizure episodes,” recurrent falls”).
Monitor choice:
- Frequent (daily), low-risk symptoms (e.g., palpitations, dizziness): Holter.
- Infrequent (weekly to monthly), low-risk symptoms (e.g., palpitations, dizziness) in compliant patients: CEM.
- Infrequent (weekly to monthly), high-risk or disabling symptoms (e.g., syncope): MCT.
- Patient compliance not reliable: MCT.
2. Screening for suspected arrhythmias in asymptomatic patients with risk factors.
Examples:
- Screening for atrial fibrillation in patients with cryptogenic stroke.
- Screening for AV block in patients with risk factors post transcatheter aortic valve replacement (TAVR).
- Screening for ventricular arrhythmias in patients with certain cardiomyopathies or inherited cardiac electrical disorders.
Monitor choice:
- MCT, especially when the suspected arrhythmia is high-risk or the diagnosis of arrhythmia requires immediate attention (e.g., anticoagulation therapy in patients with prior stroke, or AV block in patients post TAVR).
3. Evaluation of the burden, severity, or pattern of a known arrhythmia, or its response to treatment.
Examples:
- Assessment of burden and pattern of atrial fibrillation (paroxysmal or persistent) before or after treatment (drugs or ablation).
- Assessment of ventricular rate control during atrial fibrillation before or after treatment.
- Burden of PVCs or PACs before or after treatment (drugs or ablation).
- Evaluation of severity of sinus node dysfunction (sinus bradycardia, chronotropic incompetence) before or after starting certain drugs.
- Evaluation for progression of AV block (first-degree or Wenckebach second-degree AV block) before or after starting certain drugs.
- Evaluation of sinus tachycardia (e.g., inappropriate sinus tachycardia, postural orthostatic tachycardia syndrome).
Monitor choice:
- Burden of atrial fibrillation: Holter or MCT (MCT enables therapeutic intervention during ongoing monitoring).
- Rate control during atrial fibrillation: Holter or MCT (MCT enables therapeutic intervention during ongoing monitoring).
- Burden of PACs/PVCs: Holter.
- Sinus bradycardia, chronotropic incompetence, AV block, sinus tachycardia: Holter.
- Adequacy of ventricular rate control during atrial fibrillation: Holter or MCT (MCT enables therapeutic intervention during ongoing monitoring).
4. Evaluation of the relationship between a known arrhythmia and symptoms to determine necessity of intervention.
Examples:
- Assessment of relationship of sinus bradycardia or sinus pauses to symptoms.
- Assessment of relationship of Wenckebach AV block to symptoms.
- Assessment of relationship of atrial fibrillation to symptoms.
Monitor choice:
- Frequent (daily) symptoms: Holter.
- Infrequent (weekly to monthly) symptoms: MCT.
Note: the content on this site is intended solely to inform and educate medical professionals, and should not be considered a substitute for the advice or treatment of a qualified medical professional.
Unique Access to Expertise of Board-Certified
Cardiac Electrophysiologists
HRDx is the ONLY cardiac monitoring service that offers:
On-demand data clarification
On-demand EP physician curbside
On-demand professional interpretation by EP physician