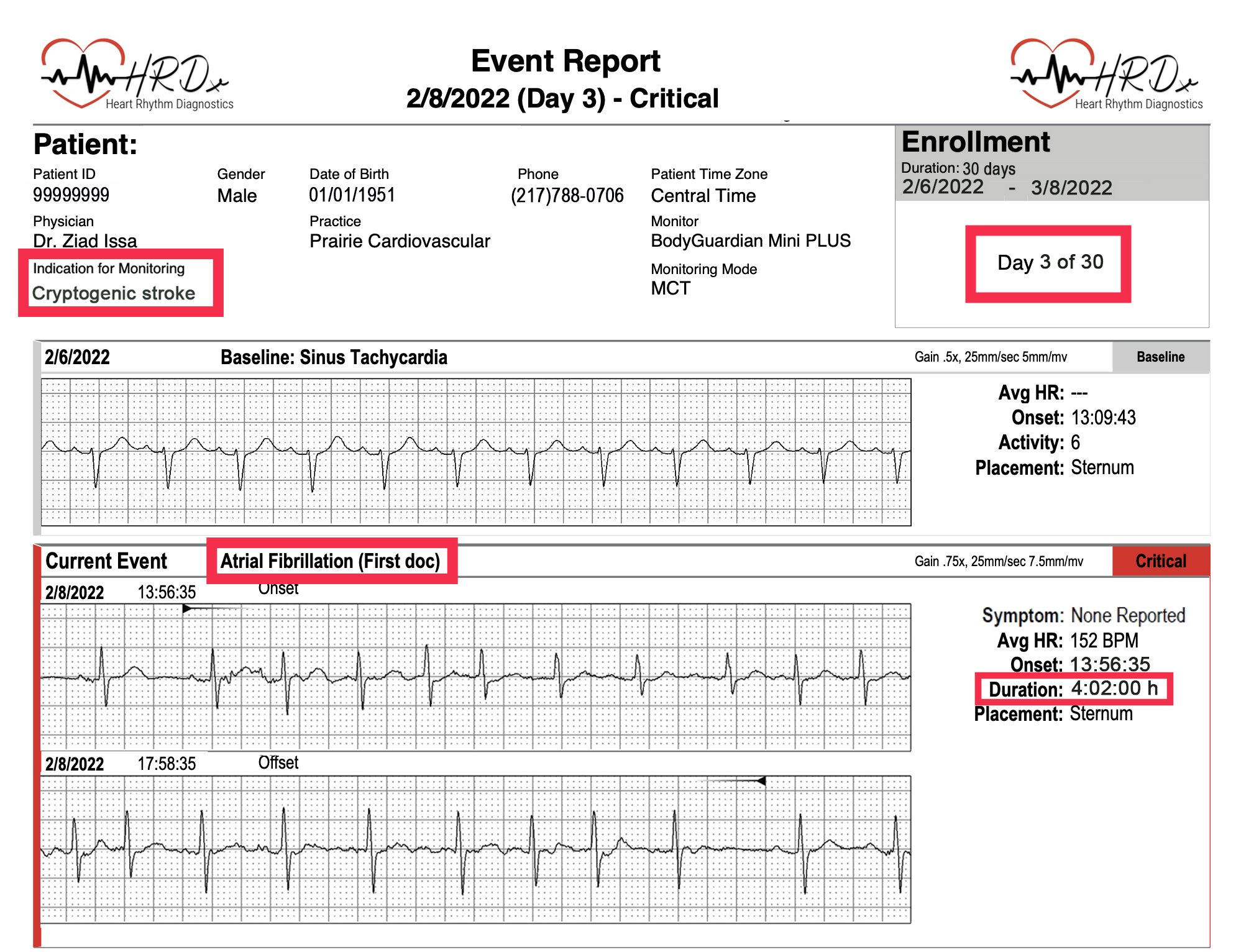
- In this example, a patient who presented with acute cryptogenic stroke was discharged from the hospital with MCT monitor for 30 days.
- AF was detected on the 3rd day of monitoring. The AF episode was asymptomatic and lasted for more than 4 hours.
- Detection of AF for the first time on MCT prompted notification of the managing medical practice within the same business day. The patient was subsequently started on oral anticoagulation and was referred to cardiac electrophysiology clinic for further management of AF.
- If the patient was monitored using only a long-term Holter, the physician would have been alerted to the detection of AF only after the completion of the monitoring period and professional report interpretation. This could result in delay of initiation of anticoagulation therapy for weeks, which could be detrimental to patient outcome.
- Also, implantation of a loop recorder is no longer necessary in this patient, since the diagnosis of AF has already been established on MCT.